
 Safe means avoiding harm, and safety is an emergent property of a well-designed system.
Safe means avoiding harm, and safety is an emergent property of a well-designed system.
Frail means infirm, poorly, wobbly and at higher risk of harm.
So we want our health care system to be a FrailSafe Design.
But is it? How would we know? And what could we do to improve it?
About ten years ago I was involved in a project to improve the safety design of a specific clinical stream flowing through the hospital that I work in.
The ‘at risk’ group of patients were frail elderly patients admitted as an emergency after a fall and who had suffered a fractured thigh bone. The neck of the femur.
Historically, the outcome for these patients was poor. Many do not survive, and many of the survivors never returned to independent living. They become even more frail.
The project was undertaken during an organisational transition, the hospital was being ‘taken over’ by a bigger one. This created a window of opportunity for some disruptive innovation, and the project was labelled as a ‘Lean’ one because we had been inspired by similar work done at Bolton some years before and Lean was the flavour of the month.
The actual change was small: it was a flow design tweak that cost nothing to implement.
First we asked two flow questions:
Q1: How many of these high-risk frail patients do we admit a year?
A1: About one per day on average.
Q2: What is the safety critical time for these patients?
A2: The first four days. The sooner they have hip surgery and are able to be actively mobilise the better their outcome.
Second we applied Little’s Law which showed the average number of patients in this critical phase is four. This was the ‘work in progress’ or WIP.
And we knew that variation is always present, and we knew that having all these patients in one place would make it much easier for the multi-disciplinary teams to provide timely care and to avoid potentially harmful delays.
So we suggested that one six-bedded bay on one of the trauma wards be designated the Fractured Neck Of Femur bay.
That was the flow diagnosis and design done.
The safety design was created by the multi-disciplinary teams who looked after these patients: the geriatricians, the anaesthetists, the perioperative emergency care team (PECT), the trauma and orthopaedic team, the physiotherapists, and so on.
They designed checklists to ensure that all #NOF patients got what they needed when they needed it and so that nothing important was left to chance.
And that was basically it.
And the impact was remarkable. The stream flowed. And one measured outcome was a dramatic and highly statistically significant reduction in mortality.
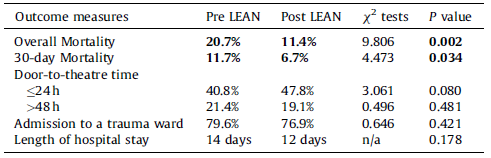
The full paper was published in Injury 2011; 42: 1234-1237.
We had created a FrailSafe Design … which implied that what was happening before was clearly not safe for these frail patients!
And there was an improved outcome for the patients who survived: A far larger proportion rehabilitated and returned to independent living, and a far smaller proportion required long-term institutional care.
By learning how to create and implement a FrailSafe Design we had added both years-to-life and life-to-years.
It cost nothing to achieve and the message was clear, as this quote is from the 2011 paper illustrates …
What was a bit disappointing was the gap of four years between delivering this dramatic and highly significant patient safety and quality improvement and the sharing of the story.
What is more exciting is that the concept of FrailSafe is growing, evolving and spreading.