
At last the light appears to be visible at the end of the tunnel for Covid-19 in the UK. And we have our fingers-crossed that we can contemplate getting back to business as usual. What ever that is.
For the NHS, attention will no doubt return to patient access targets. The data has continued to be collected, processed and published for the last 16 months, so we are able to see the impact that the Covid-19 epidemic has had on the behaviour of the hospital-based emergency system. The Emergency Departments.
The run chart below shows the monthly reported ED metrics for England from Nov 2010.
The solid grey line is the infamous 4 Hr target – the proportion of ED attendances that are seen and admitted or discharged within 4 hours. It reveals that the progressive decline over the last decade improved during the first and second waves. And if we look for plausible causes we can see that the ED attendances dropped precipitously (blue dotted line) in both the first and second waves. We dutifully “Stayed at Home to Protect the NHS and Save Lives”.
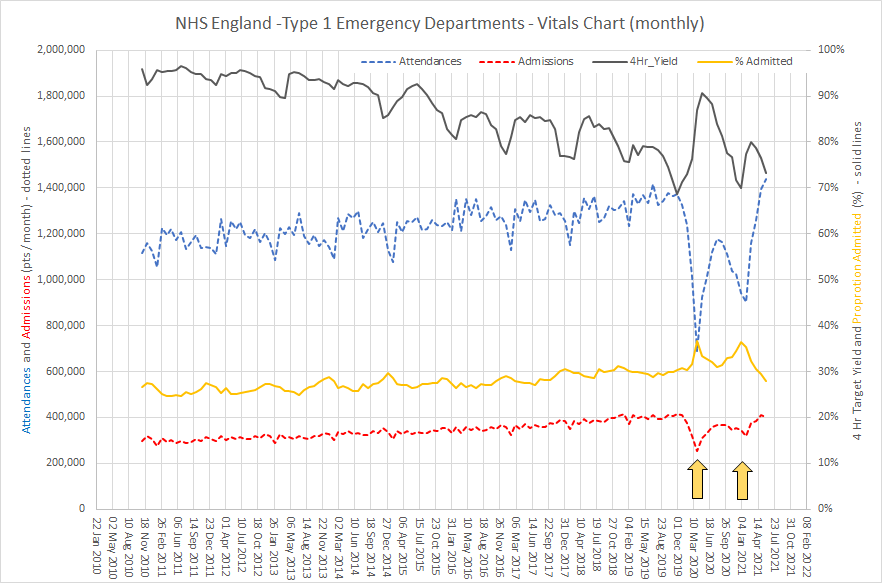
The drop in ED attendances was accompanied by a drop in ED admissions (dotted red line) but a higher proportion of those who did attend were admitted (solid orange line) – which suggests they were sicker patients. So, all that makes sense.
And as restrictions are relaxed we can see that attendances, admissions, 4 Hr yield and proportion admitted are returning to the projected levels. Business as Usual.
Up to March 2021 the chart says that 70-75% of patients who attend ED did not need to be admitted to hospital. So this begs a raft of questions …
Q1: What is that makes nearly 35,000 people per day to go to ED and then home?
Q2. How can the ED footfall drop by 50% almost overnight?
Q3. Where did those patients go for the services they were previously seeking in ED?
Q4. What were their outcomes?
Q5. What are the reasons they were choosing to go to ED rather than their GP before March 2020?
Q6. How much of the ED demand is spillover from Primary Care?
Q7: How much of the ED workload is diagnostic testing to exclude serious illness?
Q8: What lessons can be learned to mitigate the growing pressure on EDs?
Q9: Can urgent care services for this 70% be provided in a more distributed way?
And if we can do drive-thru urgent testing during Covid-19 and we can do and drive-thru urgent treatment during Covid-19 then perhaps we can do more drive-thru urgent care after Covid-19?