The first step in a design conversation is to understand the needs of the customer.
It does not matter if you are designing a new kitchen, bathroom, garden, house, widget, process, or system. It is called a “needs analysis”.
Notice that it is not called a “wants analysis”. They are not the same thing because there is often a gap between what we want (and do not want) and what we need (and do not need).
The same is true when we are looking to use a design-based approach to improve something that we already have.
This is especially true when we are improving services because the the needs and wants of a service tend to drift and shift continuously, and we are in a continual state of improvement.
For design to work the “customers” and the “suppliers” need work collaboratively to ensure that they both get what they need.
Frustration and fragmentation are the symptoms of a combative approach where a “win” for one is a “lose” for the other (NB. In absolute terms both will end up worse off than they started so both lose in the long term.)
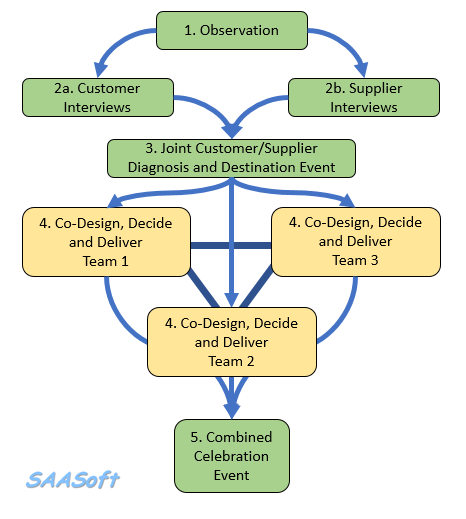
And there is a tried and tested process to collaborative improvement-by-design.
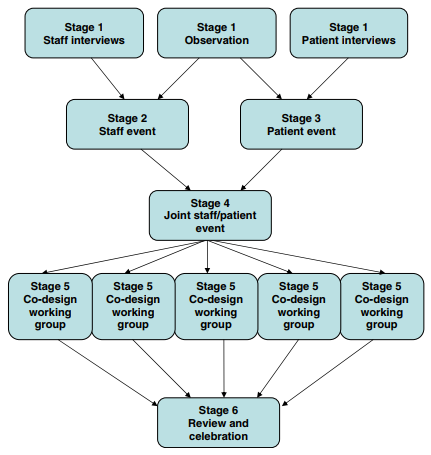
One version is called “experience based co-design” (EBCD) and it was cooked up in a health care context about 20 years ago and shown to work in a few small pilot studies.
The “experience” that triggered the projects was almost always a negative one and was associated with feelings of frustration, anxiety and disappointment. So, the EBCD case studies were more focused on helping the protagonists to share their perspectives, in the belief that will be enough to solve the problem. And it is indeed a big step forwards.
It has a limitation though. It assumes that the staff and patients know how to design processes so that they are fit-4-purpose, and the evidence to support that assumption is scanty.
In one pilot in mental health, the initial improvement (a fall in patient and carer complaints) was not sustained. The reason given was that the staff who were involved in the pilot inevitably moved on, and as they did the old attitudes, beliefs and behaviours returned.
So, an improved version of EBCD is needed. One that is based on hard evidence of what works and what does not. One that is also focused on moving towards a future-purpose rather than just moving away from past-problems.
Let us call this improved version “Evidence-Based Co-Design“.
And we already know that by a different name:
Health Care Systems Engineering (HCSE).