
The last year has been dominated by one theme – the SARS-2-CoV global pandemic. It has been a roller coaster ride of ups and downs and twists and turns, often in darkness and accompanied by the baleful drone of doom-mongers and naysayers. But there have also been bright flashes of insight that have illuminated the way and surges of innovation that have carved new designs out of old paradigms.
What we are experiencing is the evolution of a complex adaptive system and what we are seeing is the emergence of a new normal.
Almost nothing will be the same again.

The diagram above tells many inter-weaved story threads that cannot be untangled. Two Chapters are complete – CRC and UTC. We are just starting Chapter 3.
The first Thread of Tragedy is shown by the red dotted line. It is the number of daily COVID-19 associated deaths reported in the UK. The total stands at just over 127,000 which is a more than enough to fill the whole of Wembley Stadium. And a lot more.

The solid red line on the diagram is the result of removing the 7-day oscillation caused the the reporting process which opts to take weekends off.
COVID-19 is busy 24 x 7.
The first reported COVID-19 death in the UK was in the first week of March 2020. The WHO declared a global pandemic the following week, and the UK implemented the first part of a national lock down the week after. It closed some pubs in London. The need for speed was because hospital admissions and deaths were growing exponentially. As the chart shows – deaths were doubling every few days.
The Chancellor’s Magic Blank Chequebook appeared and several Nightingales were rapidly assembled to absorb the predicted storm surge. However, critically ill patients require specialised equipment and highly trained staff – and those necessities were already in short supply. As was the personal protective equipment (PPE) the front-line staff needed to keep them safe.
The Nightingales were never going to be able to sing. It was a doomed design from Day #1.
The bigger problem was the millions of potentially infectious people who would get poorly but not unwell enough to go to hospital. What was the national plan for them? It seemed that there wasn’t one. So, we created our own. The COVID Referral Centre. CRC.
This was Chapter One and the story of that has already been shared here.
The CRC was an innovative drive-thru design and a temporary solution that was conceived, commissioned, constructed and opened in 3 weeks (the red box at the top of the first diagram). It worked as designed and it was disassembled, as planned, at the predicted end of the First Wave (the orange box at the top of the first diagram).
What happened next is even more interesting. We had demonstrated, by doing it, that a drive-thru design was feasible and now we had a new challenge. Most of the elective and urgent services had been mothballed to free up space and staff to fight the First Wave. And we had no clear picture what would happen if lock down restrictions were released. The Nightingales were held in readiness. An expensive and ineffective insurance policy.
Could the drive-thru design be used for a handful of small, temporary urgent treatment centres (UTCs)?
A key lesson from the CRC was the critical importance of managing the inflow to avoid a traffic jam of anxious and potentially very poorly people. We solved this using an electronic triage and referral app that was rapidly designed, developed and delivered for the opening of the CRC. Doing that took a whole week using the JEDI method (Just ‘Effing Do It) also known as Agile.
By August 2020 things were getting back to sort-of-normal. People were having summer holidays. Schools and universities were concocting elaborate plans to re-open in the autumn. And we were thinking ahead to Winter 2020 and the prospect of seasonal flu on top of a possible resurgence of COVID. The much-feared Second Wave.
So, just before the CRC was decommissioned we took the opportunity to measure how many people could be vaccinated in an innovative drive-thru compared with a conventional walk-in. An important constraint was we did not want queues of vulnerable elderly people inside or outside. This time we had the luxury of being able to map and measure the process properly and it revealed that the drive-thru option was feasible.
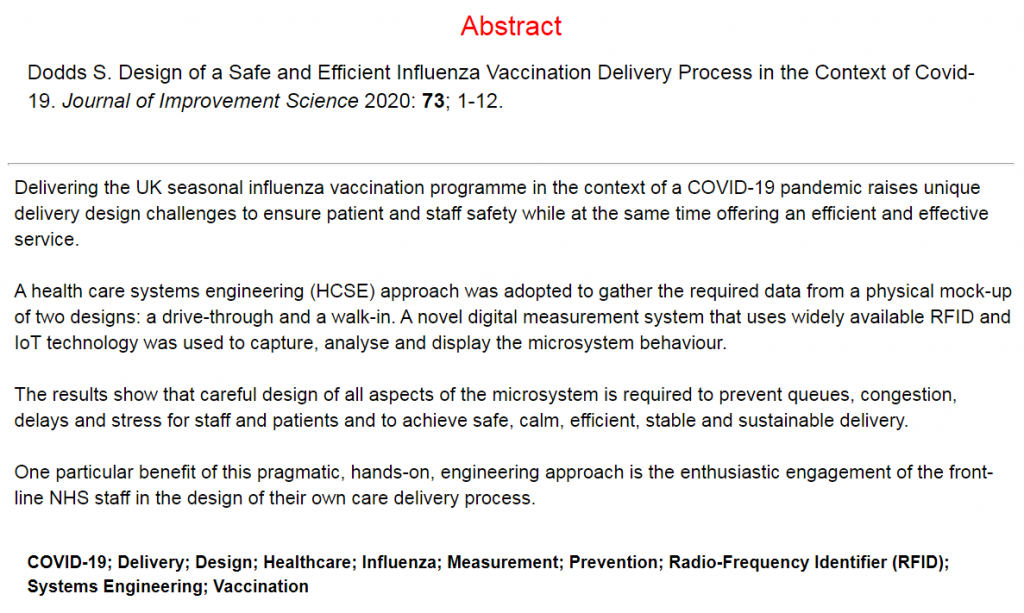
We now had the information we needed to design a high efficiency flow scheduler which would set the rate at which patients could arrive without causing queues and chaos, and at the same time make good use of the available and valuable resources.
The next design question we had to answer was “How will the booking be done?” and the immediate answers offered were “on-line” and “by the patient”.
But, this was not how the CRC worked. In that service the patient had to speak to a GP who assessed their symptoms and, if deemed necessary, referred them electronically to the CRC for a face-2-face assessment. The e-referral app was designed to limit the number of referrals to prevent a traffic jam and it also automatically assigned the next available free slot to make best use of the resources. There was no patient choice.
The other question that spun out of this exercise was “If patients could book their own appointments for a routine flu jab then could they refer themselves to a drive-thru urgent treatment centre?”
Now we were shaking the trees a bit too hard. The general consensus was “No“. But why not? Surely the patient is best placed to decide how urgent they feel their problem is? And anyway, an online self-referral can be quickly screened and any inappropriate ones addressed proactively. It is probably a better design than a walk-in service.
So, we decided to design a prototype online self-referral system and we looked on the Web for ideas that solved a similar “niggle” of being able provide convenient 24 x 7 online access to a traditional face-to-face 9-5 Mon-Fri service. Rather like the niggle of trying to get an urgent appointment at your GP practice. Or the niggle of finding an increasingly rare Post Office to go to and to get the right postage stamps for an urgent big letter / small parcel.
We discovered that the postage stamp niggle had been solved with an online app for a pay-and-print-postage-label. So, that gave us a validated design to start from.
All this digital innovation was going on during the Blue Period on the first diagram, along with the planning of a cluster of small, temporary, drive-thru UTCs placed in more convenient locations for patients. And by the time the whole caboodle was ready-to-roll it was apparent that the feared Second Wave was building momentum.
The drive-thru UTC service opened its gates in early October 2020 and only four weeks later the nation was commanded to lock down for a second time. The return of pupils to schools and students to university had created the perfect COVID incubator and the emergence of a hyper-contagious Mutant. The first diagram shows when the ‘fire-break’ lock down was eased, and when the Mutant exploded out of its cage, wiped out Christmas and doubled the UK death toll.
But, the drive-thru UTCs weathered the winter storms – figuratively and literally. They valiantly delivered a much needed service while the hospitals were swamped with a third tsunami of critically ill. The NHS was better prepared this time, which is just as well because the Third Wave was much bigger than the First.
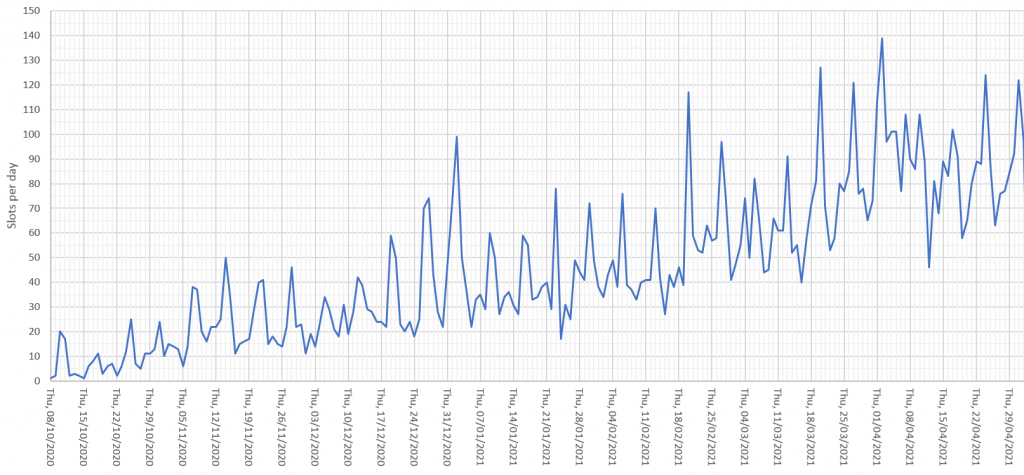
And the data the UTCs collected themselves showed that the prototype self-referral app worked as designed. We have seen gradual adoption over the seven months since it was first piloted (see below). The day-to-day variation is not random. The weekly spikes on the chart coincide with weekends when GP practices are shut and A&Es are busy dealing with accidents and emergencies (not anyone and everything).
So what does the future hold?
When COVID is just a bad/sad memory and the NHS is grappling with the elephantine challenge of post-COVID recovery amidst yet another re-disorganisation, would a more permanent drive-thru urgent care service be a viable service delivery option?
Based on the hard evidence shown I would say “Yes“.
Necessity is the Mother of Invention.
Engineers Design Things to be Fit-for-Purpose.