
 [Beep] Bob’s computer alerted him to Leslie signing on to the Webex session.
[Beep] Bob’s computer alerted him to Leslie signing on to the Webex session.
<Bob> Good afternoon Leslie, how are you? It seems a long time since we last chatted.
<Leslie> Hi Bob. I am well and it has been a long time. If you remember, I had to loop out of the Health Care Systems Engineering training because I changed job, and it has taken me a while to bring a lot of fresh skeptics around to the idea of improvement-by-design.
<Bob> Good to hear, and I assume you did that by demonstrating what was possible by doing it, delivering results, and describing the approach.
<Leslie> Yup. And as you know, even with objective evidence of improvement it can take a while because that exposes another gap, the one between intent and impact. Many people get rather defensive at that point, so I have had to take it slowly. Some people get really fired up though.
<Bob> Yes. Respect, challenge, patience and persistence are all needed. So, where shall we pick up?
<Leslie> The old chestnut of winter pressures and A&E targets. Except that it is an all-year problem now and according to what I read in the news, everyone is predicting a ‘melt-down’.
<Bob> Did you see last week’s IS blog on that very topic?
<Leslie> Yes, I did! And that is what prompted me to contact you and to re-start my CHIPs coaching. It was a real eye opener. I liked the black swan code-named “RC9” story, it makes it sound like a James Bond film!
<Bob> I wonder how many people dug deeper into how “RC9” achieved that rock-steady A&E performance despite a rising tide of arrivals and admissions?
<Leslie> I did, and I saw several examples of anti-carve-out design. I have read though my notes and we have talked about carve out many times.
<Bob> Excellent. Being able to see the signs of competent design is just as important as the symptoms of inept design. So, what shall we talk about?
<Leslie> Well, by co-incidence I was sent a copy of of a report entitled “Understanding patient flow in hospitals” published by one of the leading Think Tanks and I confess it made no sense to me. Can we talk about that?
<Bob> OK. Can you describe the essence of the report for me?
<Leslie> Well, in a nutshell it said that flow needs space so if we want hospitals to flow better we need more space, in other words more beds.
<Bob> And what evidence was presented to support that hypothesis?
<Leslie> The authors equated the flow of patients through a hospital to the flow of traffic on a motorway. They presented a table of numbers that made no sense to me, I think partly because there are no units stated for some of the numbers … I’ll email you a picture.
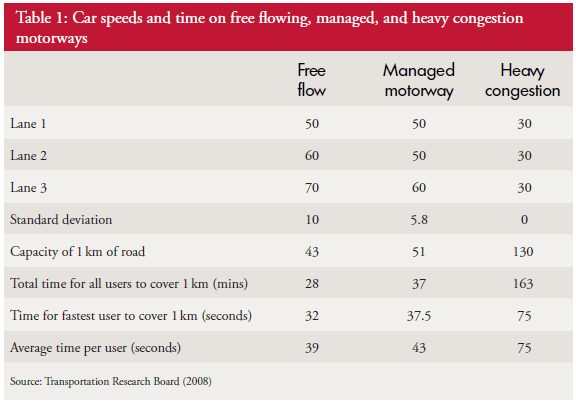
<Bob> I agree this is not a very informative table. I am not sure what the definition of “capacity” is here and it may be that the authors may be equating “hospital bed” to “area of tarmac”. Anyway, the assertion that hospital flow is equivalent to motorway flow is inaccurate. There are some similarities and traffic engineering is an interesting subject, but they are not equivalent. A hospital is more like a busy city with junctions, cross-roads, traffic lights, roundabouts, zebra crossings, pelican crossings and all manner of unpredictable factors such as cyclists and pedestrians. Motorways are intentionally designed without these “impediments”, for obvious reasons! A complex adaptive flow system like a hospital cannot be equated to a motorway. It is a dangerous over-simplification.
<Leslie> So, if the hospital-motorway analogy is invalid then the conclusions are also invalid?
<Bob> Sometimes, by accident, we get a valid conclusion from an invalid method. What were the conclusions?
<Leslie> That the solution to improving A&E performance is more space (i.e. hospital beds) but there is no more money to build them or people to staff them. So the recommendations are to reduce volume, redesign rehabilitation and discharge processes, and improve IT systems.
<Bob> So just re-iterating the habitual exhortations and nothing about using well-understood systems engineering methods to accurately diagnose the actual root cause of the ‘symptoms’, which is likely to be the endemic carveoutosis multiforme, and then treat accordingly?
<Leslie> No. I could not find the term “carve out” anywhere in the document.
<Bob> Oh dear. Based on that observation, I do not believe this latest Think Tank report is going to be any more effective than the previous ones. Perhaps asking “RC9” to write an account of what they did and how they learned to do it would be more informative? They did not reduce volume, and I doubt they opened more beds, and their annual report suggests they identified some space and flow carveoutosis and treated it. That is what a competent systems engineer would do.
<Leslie> Thanks Bob. Very helpful as always. What is my next step?
<Bob> Some ISP-2 brain-teasers, a juicy ISP-2 project, and some one day training workshops for your all-fired-up CHIPs.
<Leslie> Bring it on!
For more posts like this please vote here.
For more information please subscribe here.