
 A commonly used technique for continuous improvement is the Plan-Do-Study-Act or PDSA cycle.
A commonly used technique for continuous improvement is the Plan-Do-Study-Act or PDSA cycle.
This is a derivative of the PDCA cycle first described by Walter Shewhart in the 1930’s … where C is Check.
The problem with PDSA is that improvement does not start with a plan, it starts with some form of study … so SAPD would be a better order.
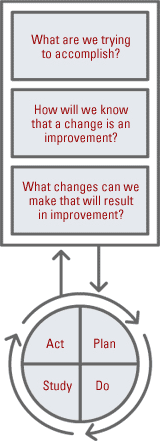 To illustrate this point if we look at the IHI Model for Improvement … the first step is a pair of questions related to purpose “What are we trying to accomplish?” and “How will we know a change is an improvement?“
To illustrate this point if we look at the IHI Model for Improvement … the first step is a pair of questions related to purpose “What are we trying to accomplish?” and “How will we know a change is an improvement?“
With these questions we are stepping back and studying our shared perspective of our desired future.
It is a conscious and deliberate act.
We are examining our mental models … studying them … and comparing them. We have not reached a diagnosis or a decision yet, so we cannot plan or do yet.
The third question is a combination of diagnosis and design … we need to understand our current state in order to design changes that will take up to our improved future state.
We cannot plan what to do or how to do it until we have decided and agreed what the future design will look like, and tested that our proposed future design is fit-4-purpose.
So improvement by discovery or by design does not start with plan, it starts with study.
And another word for study is ‘sense’ which may be a better one … because study implies a deliberate, conscious, often slow process … while sense is not so restrictive.
Very often our actions are not the result of a deliberative process … they are automatic and reflex. We do not think about them. They just sort of happen.
The image of the knee-jerk reflex illustrates the point.
In fact we have little conscious control over these automatic motor reflexes which respond much more quickly than our conscious thinking process can. We are aware of the knee jerk after it has happened, not before, so we may be fooled into thinking that we ‘Do’ without a ‘Plan’. But when we look in more detail we can see the sensory input and the hard-wired ‘plan’ that links to to motor output. Study-Plan-Do.
The same is true for many other actions – our unconscious mind senses, processes, decides, plans and acts long before we are consciously aware … and often the only clue we have is a brief flash of emotion … and usually not even that. Our behaviour is largely habitual.
And even in situations when we need to make choices the sense-recognise-act process is fast … such as when a patient suddenly becomes very ill … we switch into the Resuscitate mode which is a pre-planned sequence of steps that is guided by what are sensing … but it is not made up on the spot. There is no committee. No meetings. We just do what we have learned and practiced how to do … because it was designed to. It still starts with Study … it is just that the Study phase is very short … we just need enough information to trigger the pre-prepared plan. ABC – Airway … Breathing … Circulation. No discussion. No debate.
So, improvement starts with Study … and depending on what we sense what happens next will vary … and it will involve some form of decision and plan.
1. Unconscious, hard-wired, knee jerk reflex.
2. Unconscious, learned, habitual behaviour.
3. Conscious, pre-planned, steered response.
4. Conscious, deliberation-diagnosis-design then delivery.
The difference is just the context and the timing. They are all Study-Plan-Do.
And the Plan may be to Do Nothing …. the Deliberate Act of Omission.
And when we go-and-see and study the external reality we sometimes get a surprise … what we see is not what we expect. We feel a sense of confusion. And before we can plan we need to adjust our mental model so that it better matches reality. We need to establish clarity. And in this situation we are doing Study-Adjust-Plan-Do …. S(A)PD.