
 We form emotional attachments to places where we have lived and worked. And it catches our attention when we see them in the news.
We form emotional attachments to places where we have lived and worked. And it catches our attention when we see them in the news.
So this headline caught my eye, because I was a surgical SHO in Portsmouth in the closing years of the Second Millennium. The good old days when we still did 1:2 on call rotas (i.e. up to 104 hours per week) and we were paid 70% LESS for the on call hours than the Mon-Fri 9-5 work. We also had stable ‘firms’, superhuman senior registrars, a canteen that served hot food and strong coffee around the clock, and doctors mess parties that were … well … messy! A lot has changed. And not all for the better.
Here is the link to the fuller story about the emergency failures.
And from it we get the impression that this is a recent problem. And with a bit of a smack and some name-shame-blame-game feedback from the CQC, then all will be restored to robust health. H’mm. I am not so sure that is the full story.
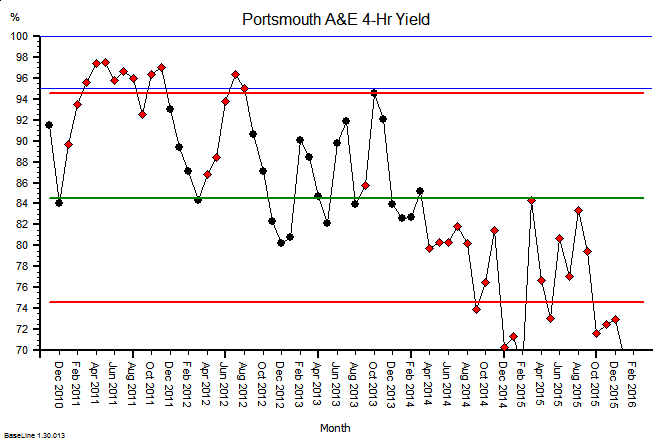 Here is the monthly aggregate A&E 4-hour target performance chart for Portsmouth from 2010 to date.
Here is the monthly aggregate A&E 4-hour target performance chart for Portsmouth from 2010 to date.
It says “this is not a new problem“.
It also says that the ‘patient’ has been deteriorating spasmodically over six years and is now critically-ill.
And giving a critically-ill hospital a “good telling off” is about as effective as telling a critically-ill patient to “pull themselves together“. Inept management.
In A&E a critically-ill patient requires competent resuscitation using a tried-and-tested process of ABC. Airway, Breathing, Circulation.
Also, the A&E 4-hour performance is only a symptom of the sickness in the whole urgent care system. It is the reading on an emotometer inserted into the A&E orifice of the acute hospital! Just one piece in a much bigger flow jigsaw.
It only tells us the degree of distress … not the diagnosis … nor the required treatment.
So what level of A&E health can we realistically expect to be able to achieve? What is possible in the current climate of austerity? Just how chilled-out can the A&E cucumber run?
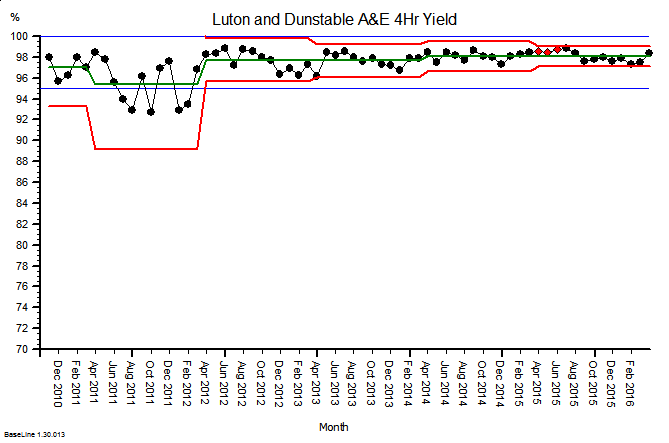
This is the corresponding A&E emotometer chart for a different district general hospital somewhere else in NHS England.
Luton & Dunstable Hospital to be specific.
This A&E happiness chart looks a lot healthier and it seems to be getting even healthier over time too. So this is possible.
Yes, but … if our hospital deteriorates enough to be put on the ‘critical list’ then we need to call in an Emergency Care Intensive Support Team (ECIST) to resuscitate us.
 A very good idea.
A very good idea.
And how do their critically-ill patients fare?
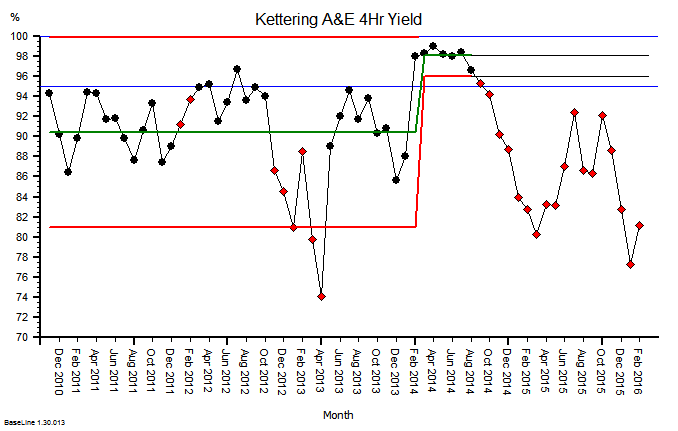
Here is the chart of one of them. The significant improvement following the ‘resuscitation’ is impressive to be sure!
But, disappointingly, it was not sustained and the patient ‘crashed’ again. Perhaps they were just too poorly? Perhaps the first resuscitation call was sent out too late? But at least they tried their best.
An experienced clinician might comment: Those are indeed a plausible explanations, but before we conclude that is the actual cause, can I check that we did not just treat the symptoms and miss the disease?
Q: So is it actually possible to resuscitate and repair a sick hospital? Is it possible to restore it to sustained health, by diagnosing and treating the cause, and not just the symptoms?
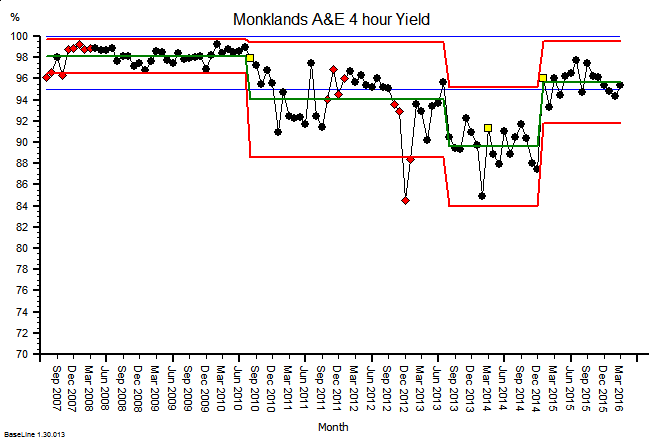 Here is the corresponding A&E emotometer chart of yet another hospital.
Here is the corresponding A&E emotometer chart of yet another hospital.
It shows the same pattern of deteriorating health. And it shows a dramatic improvement. It appears to have responded to some form of intervention.
And this time the significant improvement has sustained. The patient did not crash-and-burn again.
So what has happened here that explains this different picture?
This hospital had enough insight and humility to seek the assistance of someone who knew what to do and who had a proven track record of doing it. Dr Kate Silvester to be specific. A dual-trained doctor and manufacturing systems engineer.
Dr Kate is now a health care systems engineer (HCSE), and an experienced ‘hospital doctor’.
Dr Kate helped them to learn how to diagnose the root causes of their A&E 4-hr fever, and then she showed them how to design an effective treatment plan.
They did the re-design; they tested it; and they delivered their new design. Because they owned it, they understood it, and they trusted their own diagnosis-and-design competence.
And the evidence of their impact matching their intent speaks for itself.